
Erik Korzen DC
Guest Contributor
Reference texts: Clinically Oriented Anatomy 7th ed, K. Moore. AND Mosby’s Guide to Physical Examination, 7th ed.
Introduction
Now that we all share the same basic anatomy knowledge from the introductory post, I will dive into the first regional anatomy section. The NECK. I know that clearly, the neck is not solely it’s own region but we have to make distinctions somewhere. That being said, I will try to relate this region to the thoracic and shoulder regions as well.

To ensure I could adequately cover topics and incorporate clinical applications, we are going to look at about 2 conditions per post. That means that we will review the anatomy as well as the evaluation/diagnostic techniques that relate to the relevant anatomy. I will mention the pathophysiology of the conditions but will be keeping this based on ANATOMY.
To re-iterate the diamond shaped thinking pattern, I will provide an example of this thought process in each post. Hopefully this will start to solidify how anatomical structures are connected. When we start understanding anatomy and more specifically applying anatomy to clinical settings, we should be able to zoom IN and OUT relative ease. What I mean is that as you read through this anatomy series, you should be able to look at the macro and micro. Big picture versus minute details and tie it all together clinically.
Example: What is this pictured below? Some you may get this instantly, others may be completely lost. (Scroll to the bottom to find out!)

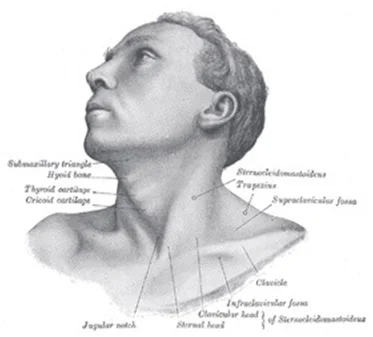
I will make an attempt to begin every post with surface anatomy. After all, this is what you first observe as a clinician.
Our thought process through an examination/evaluation should relate to how you understand anatomy. Therefore, a SUPERFICIAL to DEEP process should be utilized to assess conditions. So let's get to it!




Surface Anatomy
-thyroid cartilage
-hyoid bone
-cricoid cartilage
-thyroid gland
-sternocleidomastoid muscle (SCM)
-arteries
-veins
-trapezius muscle
-vertebrae
Carotid Artery
Vascular structures in the neck are obviously very significant due to their close proximity to the heart and brain. They can be quite evident upon observation as well, so let’s take a look.
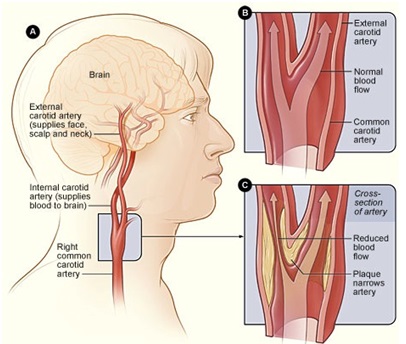
Beginning on the Left side of the body, the aortic arch will branch into the left common carotid artery and the Left subclavian artery respectively. On the Right side of the body the aortic arch gives rise to the brachiocephalic trunk (brachio- refers to arm, cephalic- refers to head) which will branch into the Right common carotid artery and Right Subclavian artery.
Looking at the picture below, we can clearly identify common carotid arteries branching into Internal and External Carotid arteries. An important distinction must be made at this point, the External Carotid artery supplies much of the face and is definitely more superficial (hence the name external). The Internal Carotid artery helps supply much of the brain, along with the vertebral arteries (remember that whole Circle of Willis thing?).

Stenosis of the common carotid or the external/internal carotids can be detrimental obviously. As depicted in the picture below, plaques can form on the lining of the arterial walls (tunica intima and media are mostly effected), leading to reduced blood flow as well as possible stroke. Essentially, this is atherosclerosis of the carotid arteries. From an ANATOMICAL standpoint, plaque accumulation in any of the carotid arteries is serious because of the structures that are downstream (face and brain).
Evaluation of the carotid arteries obviously begins with symptoms of the patient. Unfortunately, carotid artery stenosis is usually asymptomatic except for TIA (transient ischemic attacks) or ischemic strokes. So, this is where your clinical expertise comes into play. You must LISTEN to the carotid arteries with your stethoscope to assess for BRUITS (brew-eez).
First you need to find the carotid arteries. Palpate for a pulse on the anterior aspect of the sternocleidomastoid muscle, approximately at the level of the thyroid cartilage, this is known as the carotid triangle. The bifurcation from common carotid to external and internal carotids occurs around the superior aspect of the thyroid cartilage. The sternocleidomastoid muscle is a superficial structure and easily identified on surface anatomy. Common cartoid arteries can typically be palpated with superficial to moderate pressure, unless the patient has significant amounts of adipose tissue in this region.
COMPARE pulse strength bilaterally then listen with the BELL of your stethoscope bilaterally. Then move your bell slightly superiorly and inferiorly, while staying on the carotid arteries. In NORMAL arteries, essentially no sounds or minimal sounds should be heard. If you hear that whooshing sound, similar to when you take blood pressure and you hear the rushing of blood back through the brachial artery, you just found a BRUIT. Most commonly, a carotid ultrasound is performed that will provide better details of the extensiveness of the stenosis.
There it is: the anatomy of carotid artery stenosis. Let’s take a look at one more condition for this post.
Thyroid Gland
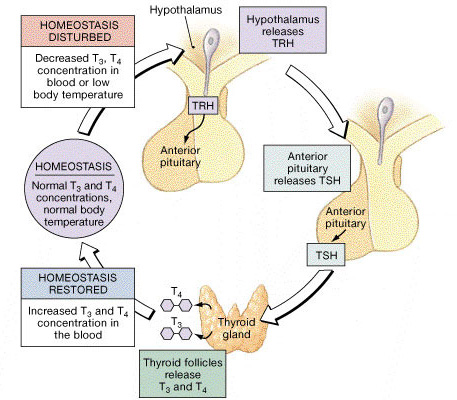
The thyroid gland is a complex and important endocrine structure located in the anterior neck. Physiologically, this gland is involved in producing T3/T4 hormones and is directly effected by the anterior pituitary gland, which is itself directly effected by the hypothalamus. Refer to the
feedback loop
for a visual representation of this.
The thyroid gland, although it shares the same name as the thyroid cartilage, is actually located inferior to the cartilage. The Right and Left lobes can normally be palpated in patients that are not too overweight. The 2 lobes are connected via an isthmus, located at approximately the 2nd-4th tracheal rings anteriorly and 5th cervical vertebra posteriorly. Check out the anatomical location of the thyroid gland:
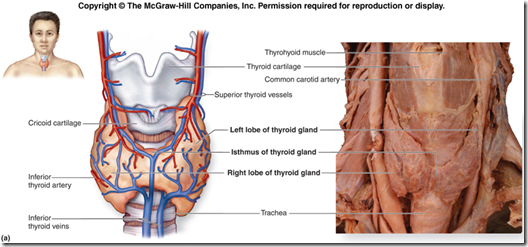
Other important structures near the thyroid gland are the common carotid arteries, trachea, cricoid cartilage. Important muscular structures include thyrohyoid, sternohyoid and sternothyroid muscles. Important vascular structures lie superficial to the thyroid gland itself, due to the organ’s role in the endocrine system. The superior thyroid artery is a branch of the external carotid artery, and the Left and Right superior thyroid arteries will typically divide into an anterior and posterior branches which will then anastamose with each other as well as the inferior thyroid artery. The inferior thyroid artery is a branch of the thyrocervical trunk which is a branch of the subclavian artery.

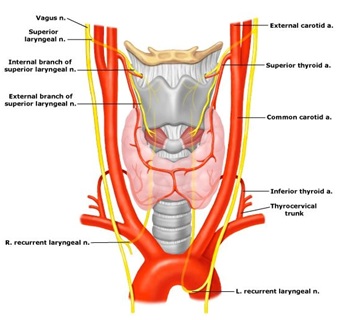
Sympathetic innervation is provided by the superior/middle/inferior cervical ganglia and the parasympathetic innervation is provided by the vagus nerves. The superior laryngeal nerve courses near the superior thyroid artery and can be compromised during surgical procedures. The recurrent laryngeal nerve courses near the inferior thyroid artery and can again be compromised during surgical procedures.
The application of superficial to deep approach is easily illustrated through this link, check it out.
Evaluation of the thyroid gland is crucial for certain conditions and a fair amount of insight can be gained from basic physical exam technique. Please check out the link for thyroid gland examination, it is extremely helpful.
Enlargement of the gland can indicate Graves disease, Hashimotos thyroiditis or tumor. Differences in the texture of the thyroid gland can be palpated and significant changes from soft to firm should be noted if present. Additionally, bruits may be heard over part of the lobes if a patient is experiencing hyperthyroidism. This is the same sound that I just mentioned in the carotid artery stenosis portion.
Most commonly, diagnostic blood tests are performed if there is suspicion of thyroid gland abnormalities. These include measuring T3/T4 hormone levels, as well as TSH (thyroid stimulating hormone) levels.
Conclusion
Let’s take a final look at that diamond-shaped thought process that some of you may not fully understand yet. The sternohyoid muscle is what we are going to use (MSK= musculoskeletal). As we think of studying human anatomy, begin with a specific structure you are interested in then broaden into the regional anatomy and entire human body and finally again narrow into the specific structure. It is important to think this way in order to fully integrate and comprehend the simplicity and intricacy of the human body. It is truly amazing!
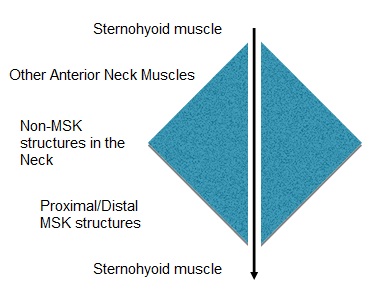
It is important to note that although I am using specific descriptors in this diagram, you can theoretically zoom IN or OUT as much as you would like.
The next post will involve two MSK conditions associated with the neck. If you have any requests/recommendations/suggestions, please feel free to let us know. This clinical anatomy series is about YOU. We want to make anatomy as clinically relevant and applicable for your practice today as possible, so input is very much appreciated.
Please feel free to connect with the author, Erik Korzen DC, if you have any questions regarding this material.

Erik Korzen, DC, NASM CES (Chiropractic Physician/Educator)
Dr. Korzen specializes in physical medicine and pain management through conservative care. He owns an evidence-based practice in IL and functions as adjunct faculty for undergrad courses in human anatomy and physiology. He has presented research at a national chiropractic conference and had an article published in ACA News monthly magazine. Dr. Korzen also has his own blog and writes for the Brookbush Institute.
Feel free to check out Dr. Korzen's LinkedIn profile for more info.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}